EAUN Fellowship experience in the Netherlands: Enhancing onco-urology nursing practice through shared learning
I was honoured to receive a European Association of Urology Nurses (EAUN) Fellowship to visit the Netherlands Cancer Institute (NKI) in Amsterdam for two weeks. This experience significantly broadened my understanding of international onco-urology practice. I am deeply grateful to the EAUN, the NKI, and all the healthcare professionals who welcomed me and generously shared their expertise.
Objective
The aim of this fellowship was to observe Nurse Practitioner (NP)-led urological services in the Netherlands and explore how these differ from UK cancer workforce models, particularly Clinical Nurse Specialist (CNS), Clinical Support Workers (CSWs) and Advanced Nurse Practitioner (ANP) roles, with a focus on scope of practice, professional autonomy, skill-mix, workforce structures, and patient pathway delivery.
Clinical experience and learning
Through clinical observation, participation in multidisciplinary team (MDT) meetings, and discussions with cancer nurses and service leaders, I explored differences in cancer nursing roles, workforce models, and patient pathway delivery between the Netherlands and the UK. The fellowship provided valuable opportunities for professional networking and knowledge exchange, enhancing my understanding of how cancer nursing practice supports service delivery within different healthcare systems.
During my fellowship at the NKI, I observed the complete uro-oncology pathway, including diagnostics, surgery, follow-up, surveillance, and survivorship care (Figure 1).
I attended renal, penile, prostate cancer, and MDT meetings, where complex cases were reviewed collaboratively by a range of healthcare professionals. These discussions highlighted the importance of coordinated multidisciplinary decision-making and demonstrated the integral role of NPs in patient management.

Clinical examples in Dutch hospitals
Penile cancer - A particularly notable experience was observing the management of penile cancer at this national referral centre. I attended procedures including partial and total penectomy, sentinel lymph node dissection, and graft reconstruction. I was also impressed by the practice of communicating histology results by telephone for patients travelling long distances, reducing the need for unnecessary hospital visits while maintaining timely, patient-centred communication.
Prostate cancer - The prostate cancer diagnostic pathway demonstrated a high level of nurse-led practice. NPs independently undertook comprehensive assessments, including PSA review, symptom evaluation, erectile dysfunction assessment, prostate ultrasound, MRI interpretation using PI-RADS scores, biopsy planning, and prostate biopsy procedures. This reflected a significant degree of clinical autonomy and procedural expertise.
I also observed NP-led follow-up clinics for patients following prostatectomy, radiotherapy, and hormonal treatment for metastatic disease. NPs independently assessed patients, managed treatment-related side effects, prescribed medication, and requested investigations such as MRI, PSMA PET scans, cystoscopy, and ultrasound examinations. This approach supported continuity of care, timely intervention, and holistic management throughout the patient journey.
Surgical Procedures - A major highlight of the fellowship was observing several advanced surgical procedures, including Robot-Assisted Laparoscopic Prostatectomy (RALP) with pelvic lymph node dissection, utilisation of Neurosafe® technology for real-time margin assessment, open Retroperitoneal Lymph Node Dissection (RPLND) for testicular cancer, and Robot-assisted Radical Cystectomy with ileal conduit formation. The cystectomy case was particularly complex due to previous chemotherapy, the presence of a horseshoe kidney and significant adhesions, demonstrating the complexity of contemporary pelvic oncology surgery.
Post-operative, survivorship and quality of life (Figure 2)
- Post-operative Care - I gained valuable experience within post-operative services, observing specialist stoma nurses managing complex post-surgical care. Their role encompassed wound assessment, stoma management, and the treatment of complications such as hypergranulation tissue. I was particularly impressed by the emphasis placed on patient education and self-management, with nurses actively supporting individuals to develop the knowledge, confidence, and practical skills required to achieve independence in stoma care and daily living activities.
- Survivorship - The survivorship model extended beyond routine clinical surveillance and focused on supporting patients throughout their transition from active treatment to long-term self-management. NPs played a key role in promoting recovery, providing ongoing support, and helping patients adapt to the long-term consequences of treatment. This approach recognised survivorship as an active process, aimed at restoring independence and empowering patients to take ownership of their ongoing health and wellbeing.
- Quality of Life (QoL) - Quality-of-life is monitored via physical and psychosocial outcomes. Follow-up care focused on identifying ongoing supportive care needs, managing the long-term effects of treatment, and addressing issues that could affect patients' overall wellbeing.
Reflections of Dutch and UK cancer role models
One of the most valuable aspects of the fellowship was observing the high level of autonomy demonstrated by NPs in the Netherlands. NPs are educated to master’s level, hold a Master of Science (MSc) qualification, and practise autonomously across the patient pathway.
Across diagnostic, treatment, and follow-up pathways, NPs were responsible for comprehensive patient assessment, reviewing investigations, undertaking procedural interventions, prescribing, requesting diagnostic tests, and managing ongoing treatment-related concerns.
These observations highlighted differences between Dutch and UK workforce models (Figure 3).
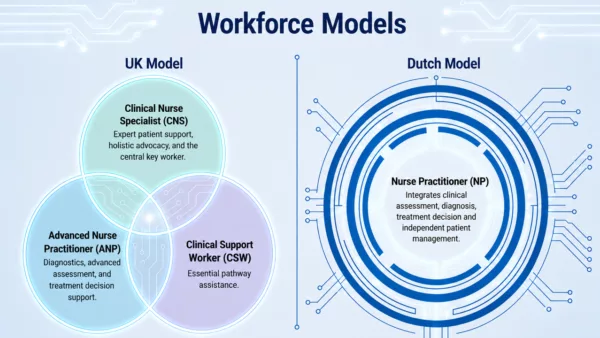
UK onco-urology services utilise a distributed workforce model in which CNSs, ANPs, and CSWs have distinct but complementary roles.
- CNSs function as the patient's key worker, providing holistic support, care coordination, patient advocacy, and continuity throughout the cancer pathway. CNS roles may range from Band 6 development posts, where nurses are building specialist knowledge and skills, to Band 7 senior CNS roles with greater autonomy, leadership, and specialist expertise.
- ANPs focus on advanced clinical practice, undertaking autonomous assessment, diagnostic investigations, treatment planning, prescribing, and clinical decision-making.
- CSWs support pathway delivery through administrative, coordination, and patient-facing activities, helping improve service efficiency and patient experience.
The UK workforce model is supported by the ACCEND (Advancing Clinical Practice through Education, Career Development and Networking) framework, which provides a structured approach to workforce development, competency progression, education, and career pathways across support worker, specialist, and advanced practice roles.
While both systems deliver high-quality patient care, they differ in how responsibilities are structured. In the UK, patient coordination and holistic support are typically provided by CNSs, while ANPs undertake advanced assessment, diagnostics, and treatment management. In contrast, the Dutch NP role integrates many of these functions within a single practitioner, reflecting differences in healthcare organisation, workforce structures, and levels of professional autonomy.
Conclusion
This fellowship has significantly influenced my understanding of cancer nursing practice, workforce development, and service delivery within Uro-oncology care. Observing Dutch NP-led pathways provided valuable insight into alternative approaches to role utilisation, autonomous practice, and patient management across the cancer pathway. The experience broadened my perspective on how different nursing workforce models can contribute to high-quality, patient-centred care, while reinforcing the importance of multidisciplinary collaboration, continuous professional development, and international learning in supporting excellence in clinical practice.
The EAUN Fellowship was both professionally and personally enriching, providing opportunities to develop international professional networks, and critically reflect on how workforce design influences patient pathways, service efficiency, and professional development. It highlighted the importance of ensuring that cancer nursing roles are utilised to their full potential to meet increasing service demands while maintaining high standards of patient care.
Most importantly, this fellowship reinforced that there is no single optimal model of care. Excellent patient outcomes can be achieved through a variety of approaches when workforce structures, professional roles, and service delivery models are aligned with local healthcare systems, available resources, and patient needs. The experience has inspired me to continue developing my expertise in cancer nursing practice and to promote collaborative learning, innovation, and knowledge sharing within uro-oncology services. I am extremely grateful to the EAUN, the NKI, and The Royal Marsden NHS Foundation Trust for supporting and enabling me to undertake this unique fellowship. Their commitment to education, professional development, and excellence in patient care made this invaluable learning experience possible.