7. PRINCIPLES OF MANAGEMENT OF NURSING INTERVENTION
MEC offer the advantage of diverting the urine to a bag, thus decreasing urine odour and protecting the skin from contact with urine. MEC may reduce the risk of complications associated with navigating the barrier protecting the urinary tract from stool. This may be especially true in the presence of liquid stool. [22,45]
7.1 Assessment including measuring
Before you start the assessment, the patient should be informed about the procedure and you must obtain informed consent from the patient.
For elderly persons, expectations of assessment and treatment may need to be modified to fit in with specific circumstances, needs, and preferences, while taking into account any loss of capacity for consent. When the healthcare professional is dealing with a frail elderly patient with urinary incontinence, collaboration with other healthcare professionals such as elderly care physicians is recommended. [3]
Assessment involves considering the patient’s individual situation, measuring and selecting the proper devices:
1. Patient situation
- Is there an indication for MEC (chapter 4)
- Are there any contraindications (chapter 4)
- Are there more suitable alternatives (chapter 4)
- Continence symptoms and history of management
- Is the patient’s clinical condition suitable
- Physical examination
i. Penile skin condition (see chapter 7)
ii. Retracted penis (see chapter 7) - Mental acuity: Is the patient able to handle the MEC (cognitive, psychological) or if not, is a relative or healthcare professional able to assist
- Dexterity and Mobility - is the patient able to handle the MEC in case of impaired mobility or problems with hand/finger movement
- Home environment [46,47]
- Is the product available for the patient [7]
- Is there any preference for a product by the patient
- Is the cost acceptable
2. Measuring
- Size and length
- Using measuring tools
3. Selecting
- Choice of material
- Choice of application technique
- Choice of urinary drainage bag
7.1.1 Patient situation
Each patient should be individually assessed, as there is no single product that will meet all patients’ needs. Patients must have sufficient penile length and girth, and they or their carer must be competent and willing to use the device.
The objective for fitting a MEC is to maximize the user’s quality of life. [48] Bath et al (1999) [29] stated that some nurses find the process of assessment and fitting a MEC difficult due to their embarrassment regarding the intimate nature of the procedure.
A full assessment involves the collection of data and information relating to each individual’s incontinence problems. [48] The assessment should ensure that the MEC is the most appropriate management choice and will not result in problems that deserve more active intervention.
Patients with cognitive impairment may try to remove their MEC, which will cause pain and possible tissue injury. Therefore, these patients should be carefully assessed before they are given these products. [8]
There is a definite need for compliance when using a MEC. Therefore, both patient and carer need to discuss the issue before a decision is finally made to use this device. [8]
7.1.2 Measuring
In order to find the appropriate size of the MEC, the circumference of the penis needs to be measured. The penis should be measured at the shaft where its diameter is largest in order to assess the correct size. [46] During measurement, the patient should be seated on the edge of a bed or chair with their legs slightly spread. In this free position both the scrotum and penis are in their natural anatomic orientation and can best be measured. The actual MEC size of the penis may be hard to determine if it ranges between two sizes. Should this situation occur, the patient should try both sizes at home. MEC materials are sufficiently flexible and allow a snug, but not tight fit. Many manufacturers and suppliers of MEC offer sizing guides (for example cardboard moulds or patterns), to help determine the size that will ensure safe and comfortable wear. [8,44] It is important to note that manufacturer sizes may vary, and sizing guides provided by one manufacturer should not be used for another.
Listed below are various size ranges provided by four manufacturers:
- Sauer Continence 18, 20, 22, 24, 26, 28, 30, 32, 35, 37, 40 mm
- Coloplast 21, 25, 28, 30, 35, 40 mm
- Hollister Incorporated 25, 29, 32, 36, 41 mm
- B. BRAUN 25, 29, 32, 36, 41 mm

Fig. 38. MECs in various lengths
InView Silicone Male External Catheter
(Source: Hollister Incorporated)
It is more important to determine the exact diameter of the penis to fit the correct size of the MEC than the length of the penis. All MECs currently available will fit most penis lengths, except when the penis is very small or retracted.
Nevertheless some manufactures have different lengths so the optimal size and length can be chosen.
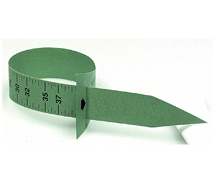
Fig. 39. Measuring device
(Source: Manfred Sauer GmbH)
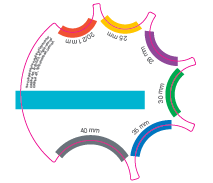
Fig. 40. Measuring device
Conveen® measuring guide
(Source: Coloplast)
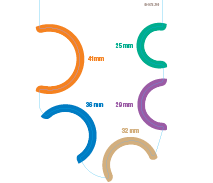
Fig. 41. Measuring device
InView Global Sizing Guide
(Source: Hollister Incorporated)
Retracted penis
Penile retraction occurs when the penis retreats inside the prepubic fat. This is a common occurrence in older men. If there is some penile retraction, the patient may be able to use a shorter length MEC. If total penile retraction is observed when the patient is sitting down, neither a standard nor short length MEC will stay in place and may fall off. [49]
Assessing penile retraction
Have the patient stand (if possible) and observe penile length. Gently press back on either side of the penis towards the pubic area to expose as much retracted length of the penis as possible. Observe the change in length and position. If the seated penis length is less than 5 cm, use a shorter length MEC. [7,49]
Special MECs are available on the market for patients with a shorter or retracted penis. Since a retracted MEC is shorter in length than a regular MEC, there is less area for the adhesive side of the catheter. Therefore, it is most important that the correct male external catheter size is selected. To apply the MEC, the patient should lie on his side. In this position, it is easier to reach most of the penis to attach the MEC. When the MEC is placed in the correct way, it can “handle” a retraction of the penis better. [7,49]
In the case of retracted penis there are some special MECs (e.g., BioDerm) or MECs with a shorter area of glue, or stronger glue. To apply the MEC, it is helpful if the patient brings the penis to an erection. The patient can do this at home if possible. Therefore, a vacuum pump could be helpful.
7.1.3 Selecting
One- or two-piece MEC
The selection of a one- or two-piece MEC is a matter of personal preference, but for reliability and ease of use, most patients prefer to use a one-piece system. However, a two-piece MEC can be beneficial for those whose glans is larger than the shaft of the penis or where the patient has developed sensitivity to the adhesives used in the one-piece systems. Select a sheath that is easy to apply, as ease of application promotes confidence in users.
External fixation enables the MEC to be removed and intermittent catheterisation to be performed, but does not offer the security of internal fixation.
Drainage bag
The choice of drainage bag is dictated by several factors:
- Reason for use
- Intended duration
- Patient mobility and activities
- Patient preference
Consideration should be given to the bag capacity and placement. Either leg or bed bags can be used.
There are different sizes of bags. A patient might use a smaller bag during the day and a larger one at night.
The leg bag, body worn bag or waist suspended bag need to be attached properly, in order to allow urine to flow into the bag without difficulty.

Fig. 42. Leg bag
Comfort Leg Bag
(Source: Manfred Sauer GmbH)

Fig. 43. Leg bag
Bendi Bag
(Source: Manfred Sauer GmbH)
The leg bag can be placed at different positions on the leg: thigh, knee (special bag needed), and under the knee. A leg bag is the best choice for ambulatory patients. The bag is most commonly fastened around the thigh or with two straps. Sleeves and belts hold the bag safely and may be more comfortable. As the urine bag fills it becomes heavier and may stretch the straps. The urine bag should not be allowed to fill to the point of discomfort, but should be emptied when 2/3 full.
When the urine bag fills it becomes heavier and may stretch the straps. The urine bag should not be allowed to fill to the point of discomfort, and should be emptied when two-thirds full.
It is recommended to change the urine bag at least once weekly, but in many hospitals, the bag is changed every time that the MEC is changed. Changing the urinary bag depends on local or national policies or standards.

Fig. 44. Example of a leg bag for a wheelchair user
Comfort Leg Bag
(Source: Manfred Sauer GmbH)
- Adjust seating for wheelchair users, if necessary, to allow better drainage.
A bed bag/night drainage bag can be used instead of a leg bag and needs to be placed below the person to permit the flow of urine. It is important to choose the drainage bag that best meets the needs of the patient. [50]
- Ensure the urine bag is of the correct size and that it is well supported to avoid dragging on the sheath.
In case of impairment of hand function or vision, the type of tap can be an important factor for patients to be as independent as possible when emptying the bag.
Testing sensitivity
- Test the product for sensitivity, bearing in mind that some patients are allergic to latex.
For a flowchart on how to select the best urinary bag for the patient please refer to:
Appendix D: Flowchart MEC - Urinary bag decision tree
7.2 Application of the MEC
Step by step procedure: see Appendix A
7.2.1 Patient preparation
It is not advisable to shave the pubic area as this can cause skin irritation, but hair can be trimmed if necessary, to prevent it being caught in the sheath. [7]
Alternatively a hole can be torn in a tissue then placed over the penis to push the hair back. Some MEC include a hair guard.
7.2.2 Applying adhesives
See Appendix A
7.2.3 Skin care and meatal cleansing
The skin should be dry and undamaged before placing the MEC onto the penis. If the skin is undamaged, normal personal hygiene is sufficient.
Skin care products
When using silicone MEC, skin care products should not be used because they will reduce the adhesiveness of the MEC (Coloplast product information). In the case of skin care problems when using non-silicone products, there are different skin care products available on the market to help keep the skin healthy. A moisturizing cream should be pH neutral, oil free, and unscented. It should be free of soap and other cosmetic ingredients. [7]
Avoidable skin care products
An oil-based moisturising cream may change the integrity of the glue and affect the adhesive leading to leakage or displacement of the MEC. Perfume, soap or other cosmetic ingredients can irritate the skin, causing fungal skin infections, skin damage or abrasions and allergies.
When skin care problems are solved, the patient can return to normal personal hygiene in most cases. The skin also has a self-healing function.
7.3 Observation of the applied MEC
Frequent monitoring of the device is needed for effective use of this product. [16]
An hour after first application and with every catheter change, the MEC should be carefully observed to see if it fits well, tubes are not kinked, and there is no leakage and no pain.
7.3.1 Skin irritation
The skin should be carefully examined for signs of soreness or irritation. This is particularly important for patients with neurological deficits, who may be unaware that the sheath is too tight or causing skin problems. [29]
Nurses must inform caregivers and patients who may not be accustomed to this type of product that skin irritation may occur. They should be advised to remove the MEC immediately if skin irritation occurs and gently wash and thoroughly dry the area to remove any residual adhesive. [29] The area should be dried and may be left open to the air unless blisters have formed and have exuded fluid. A clean non-occlusive dressing may be placed over the affected area. [29] This type of MEC should not be applied again and the incident should be reported to the clinician. The reaction should be recorded in the patient’s records. [29]
In people with reduced or no skin sensation due to spinal cord injury or multiple sclerosis, an ill-fitting MEC could cause a pressure sore or skin lesion. Therefore, in these patients, it is necessary to observe the skin once daily.
7.3.2 Leakage
If a MEC does not remain secure for a 24 hr period the likelihood is that:
- stronger adhesive is needed
- the MEC is too large
- incompatibility of products,
- incorrect application technique
- penile retraction is present
- UTI
- mobility or activity of the patient
- aggressive urinary output (occurs in cases of UTI and chemotherapy)
- sweating
- pubic hairs
- combination of the problems mentioned above
Leakage prevention
In the event of a large volume urine loss a MEC containing an anti-reflux membrane can be useful in maintaining the integrity of the adhesive and protecting against leakage.
For details on how to manage the various problems, please refer to appendix C Troubleshooting.
7.3.3 Kinking
Avoid kinking or twisting of the sheath or the drainage bag as this allows urine to pool, thereby weakening the adhesive or blocking drainage completely. [7]
7.3.4 Changing interval
Daily changes of sheaths are recommended for all users when daily hygiene is performed. When the MEC falls off or leakage occurs it should be changed more often and if this recurs the patient should be reassessed.
It is recommended that the urine bag should be changed at least once a week. In hospitals, the bag is changed every time the MEC is changed due to the risk of cross contamination. Changing the urinary bag should follow local or national policies or standards.
7.4 Removing the MEC
Remove the MEC and the tape simply by rolling them off. Usually, the adhesive comes off with the MEC when removed. However, if there is adhesive remaining it can be washed with skin care products or rubbed off. Do not remove the adhesive with solvents, such as acetone or similar substances, since this will disrupt the natural oil balance of the skin and may cause chapping and cracking, leading to inflammation. Non-solvent based adhesive remover pads are available, but water and soap are recommended. In special cases, products used in stoma care could be used. [8,43,44]
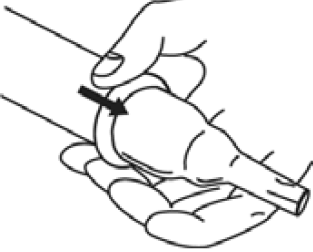
Fig. 45. MEC roll off
(Source: Manfred Sauer GmbH)
7.5 Collecting a urine sample from a MEC
Patients with symptoms such as dysuria, urgency, frequency, flank pain, costovertebral angle tenderness, suprapubic pain and fever may have a UTI and a urine sample should be sent for culture. Urine samples should be collected using a protocol that minimises contamination from the genital mucosa and perineal skin. [51] Guidelines recommend the collection of a mid-stream specimen in adults. The study by Nicolle (1988) [52] and Ouslander (1987) [53] found no difference between bacteriuria in urine collected from a clean MEC compared to urine from a sterile in-and-out (intermittent) catheter.
| How to collect a urine sample |
| 1. Meatal cleansing with water and soap |
| 2. Dry the skin carefully |
| 3. Put on a new MEC and attach a new urine bag |
| 4. Collect the urine sample from the sampling port from the first voided urine [25,52] |
| 5. Take the urine to the laboratory immediately or refrigerate the urine sample immediately after collection to prevent false results |
| Recommendations | LE | GR |
| Patients with cognitive impairment should be carefully assessed to determine if they are able to fit and manage a MEC [8] | 4 | C |
| Measure the length and the circumference of the penis at its widest point to fit the MEC in the correct way | 4 | A* |
| Assess the correct length of the inlet tube, taking into account whether the patient is a wheelchair user, a walker or bedridden | 4 | A* |
| Assess hand function of the patient and valve taps before choosing a urinary bag for the MEC | 4 | C |
| Shorten pubic hair to prevent it being caught in the sheath | 4 | C |
| Skin should be observed before fitting a MEC | ||
| Skin should be observed after MEC is applied | 4 | C |
| Avoid creams and powders as they affect the adhesion of the MEC [54] | 4 | C |
| Hydrocolloid could help healing if skin is damaged | 4 | C |
| Skin should be observed after removing the MEC | 4 | C |
| Change the MEC daily [23,55] | 4 | B |
| Use a non-sterile urinary bag | 4 | C |
| Secure the urinary bag to allow free urine flow | 4 | C |
| Empty the urinary bag when two-thirds full | 4 | C |
| Change the urinary bag at least once weekly or follow local policy. | 4 | C |
| Follow protocols for collecting urine samples for urine culture from a MEC [51-53] | 2a | B |
| Collect the first voided urine within an hour after MEC change from the sampling port in the drainage tubing [51-53] | 2a | B |
An A* grade recommendation is a strong recommendation despite level 4 evidence.