10. Preparation and administration of intravesical therapy
Before starting the intravesical instillation, some general aspects should be considered. In this chapter, we describe aspects related to patients, medication used and administration procedures.
10.1 Patient assessment
Prior to initial and subsequent administration of intravesical therapy, the patient should be assessed before and after all instillations with regard to the following:
- Overall health status
- Specific urological health status
- Ability to understand the procedure
- Ability to comply with the treatment plan
- Understanding treatment side effects and potential complications
| Recommendations | LE | GR |
|---|---|---|
| Confer with urologist if symptoms of local or systemic UTI. | 4 | C |
| Do not use dipstick to rule out UTI [20]. | 3 | B |
10.2 Pre-procedure
Assessing the patient prior to commencing each intravesical therapy aims to:
- Highlight any potential risks or complications from treatment.
- Identify any individual patient requirements that may affect compliance, concordance and efficacy of treatment.
- Help manage patient expectations.
- Highlight any aspects requiring specialist referral or further assessment.
Table 6 presents the most common problems during patient assessment. A common tool for undertaking nursing assessment is using a model of nursing care such as the Roper, Logan and Tierney Activities of Daily Living model of nursing assessment [51]. This assessment is undertaken at the outset of treatment and highlights the normal situation for patients and identifies the changes that occur during their illness.
Table 6. Common problems identified during assessment and nursing interventions
| Maintaining a safe environment | |
|---|---|
| Finding | Nursing interventions |
| Inability to mobilise to/from toilet | Consider indwelling catheter with clamp/valve for the duration of the dwell time. |
| Neurological impairment | Consider keeping patient in clinic for the duration of the dwell time. |
| History of traumatic/difficult catheterisation causing urethral bleeding | Catheterise with extra care or use more lubricant than usual or consider an alternative catheter or more experienced personnel. |
| Communication | |
|---|---|
| Finding | Nursing interventions |
| Inability to understand rationale for treatment | Provide an explanation and written information to carers/families/interpreters where appropriate. |
| Memory or mental health problems | Ensure that a carer is available or keep the patient in hospital/clinic for the duration of the dwell time. |
| Inability to understand the importance of holding urine for dwell time | Consider indwelling urethral catheterisation with clamp/valve for the duration of the dwell time. |
| Eating, drinking and smoking | |
|---|---|
| Finding | Nursing interventions |
| The role of nutrition; vegetables | Inform that increasing consumption of raw cruciferous vegetables (75 g) could be a strategy to provide further protection against risk of recurrence, particularly those who receive BCG. [52]. |
| Patient unable/unwilling to restrict fluid intake prior to instillation | Advise the patient that restricting fluid intake may help to maintain intravesical therapy for the desired time and prevent over dilution of the drug during dwell time [53]. |
| Patient unwilling to drink excess fluid after the dwell time | Advise the patient that increased fluid intake after the dwell time may help eliminate intravesical therapy agents from the bladder and reduce the risk of side effects. |
| Patient is a current smoker | Inform the patient that smoking reduce the efficacy of BCG immunotherapy [54, 55]. |
| Elimination | |
|---|---|
| Finding | Nursing interventions |
| Lower urinary tract symptoms (LUTS) | Assess LUTS in women with the ICIQ FLUTS score and in men with the International Prostate Symptom Score (IPSS). |
| Storage symptoms | Consider management of storage symptoms that are likely to worsen during treatment (e.g. anticholinergics or containment products) [56]. |
| Obstructive symptoms (affecting elimination of intravesical therapy) | Consider postmicturition bladder scan to ensure intravesical therapy agents are eliminated from the bladder. In patients with residual urine, consider α blockers, 5α-reductase inhibitors, intermittent self-catheterisation and surgical management. |
| Signs/symptoms of UTI | Send urine for culture and withhold treatment. |
| Urinary incontinence | Consider containment products or indwelling urethral catheterisation for the duration of the dwell time. |
| Controlling body temperature | |
|---|---|
| Finding | Nursing interventions |
| High fever (> 38.5°C) | Discuss this with the doctor and consider interruption of treatment – treatment not to be administered. |
10.3 Informed consent
Depending on local regulations, some centres may require patients to sign a consent form, whereas others may accept verbal consent. Before administering treatment, it is important that the nurse be confident that the patient has been informed regarding the benefits and risks of intravesical instillation.
10.4 Preparation of bladder instillation medication
Bacillus Calmette-Guérin should not be prepared in areas in which intravenous drugs are prepared, because nosocomial infections have been reported in patients receiving parenteral drugs that were prepared in areas in which BCG was prepared [57].
Procedure
Follow the directions on the manufacturer’s package insert (SmPC) for proper preparation of MMC and BCG.
Dosage
The dosage range for MMC is 20–60mg. The most frequent dose is 40mg. The dosage of BCG is based on the number of colony forming units (CFUs), which depends on the specific BCG strain and varies between 1 to 8 x 108 and 109 CFUs. In clinical practice, milligram dosages are often used (range 40-120mg, depending on the strain) [58].
10.4.1 Medication pre-procedure
If the patient has pre-existing storage symptoms, anticholinergics may be effective [59]. Caution must be used in patients with conditions that could be aggravated by this medication, such as angle-closure glaucoma, benign prostatic hyperplasia and cardiac disease. If anticholinergics are ineffective or contraindicated, β agonists may be used. A study found no benefit in using oxybutynin routinely as prophylaxis against urinary symptoms during BCG therapy [60]. If concerns persist regarding incomplete emptying, the patient should be counselled to keep the catheter in for the duration of treatment.
10.4.2 Analgesics
There is no contraindication for non-steroidal anti-inflammatory agents.
10.4.3 Antibiotics
There is no evidence that concurrent use of antibiotics decreases the efficacy of BCG or MMC, but if a patient is being treated with antibiotics, starting bladder instillation should be discussed with the prescribing physician.
10.4.4 Diuretics
When patients are prescribed diuretics as part of their regular medication, the need to refrain from taking prescribed diuretics must be verified with the patients’ urologist, because this is a patient-specific issue. Instruct the patient to minimise fluid intake in the 3 to 4 hours before treatment to minimise urine production during treatment [61]. This may also help improve the patient’s ability to retain the instilled medication for the prescribed dwell time.
10.5 Administration of intravesical instillation
10.5.1 Positioning of the patient
The structure of an empty bladder allows the bladder wall to directly interact with the intravesical medication and, therefore, patients should be encouraged to remain as mobile as usual. Some hospitals request patients to rotate from side to side every 15 minutes (the ‘rotisserie’ method) to improve drug contact with bladder mucosa [38, 62]. However, It has been demonstrated that there is no difference in recurrence rates between the rotisserie and non-rotisserie methods during treatment with BCG
[63]. This reinforces the idea that contact with the bladder wall is sufficient for the medication to be effective.
For practical reasons, the catheter should be inserted while the patient is in the supine position. If there is no risk of incontinence, no further mobility restrictions are necessary. Mobility is encouraged over bed rest.
10.5.2 Cleaning of the meatus
Routine daily personal hygiene is all that is needed to maintain meatal hygiene [64-68]. Trials of various cleaning agents, such as chlorhexidine and saline, have failed to reduce bacterial growth rate, therefore, soap and water is sufficient to achieve effective meatal cleaning [11, 68, 69].
10.5.3 Instillation equipment
Chapter 7 discusses the importance of safe handling of both BCG and MMC. Because a closed system is highly recommended, nurses are advised to use ready-to-use kits. Currently, ready-to-use packages are available that contain a closed system transfer device intended solely for intravesical instillations. These kits can be prepared without the need for a biological safety cabinet, thus simplifying the logistics of the procedure. The kits can also be stored on the ward where the instillation takes place.
If ready-to-use medication is not available in the area, it must be prepared in advance. Check the Summary of Product Characteristics (SmPC) for information on stability and how long the medication remains viable after reconstitution.
In this case, it is mandatory to either have access to a biological safety cabinet or use a closed system to reconstitute the medication. Such systems are airtight, leakage-resistant and utilise membrane technology. If the above-mentioned systems are unavailable, it is recommended to prepare the medication in a pharmacy department equipped with a biological safety cabinet.
10.5.4 Catheter type and size
Where possible an intermittent catheter should be used. Some considerations for the choice of catheter for the intravesical instillation include:
- The smallest size possible, such as CH10, or CH12 should be used to prevent causing pressure and injuring urethral tissue [68], as well as to prevent excessively rapid instillation.
- Hydrophilic or prelubricated catheters decrease the risk of discomfort, trauma and post-catheterisation infection [70-72].
- Luer lock catheters (Figure 1) reduce the risk of spillage by maintaining a closed system. Some intermittent catheters have the luer lock end integrated, whereas indwelling catheters require an adaptor attached prior to the instillation procedure. Some of the MMC and BCG products in ‘ready-to-use packaging’ are equipped with the luer lock system.
- The first choice for instillation is an intermittent catheter. An indwelling catheter should only be placed when there is a clear indication. The indwelling catheter should not stay in place any longer than necessary [68].
10.5.5 Lubricant
For non-hydrophilic catheters, 10–15ml of lubricant with lidocaine should be used [68, 73].
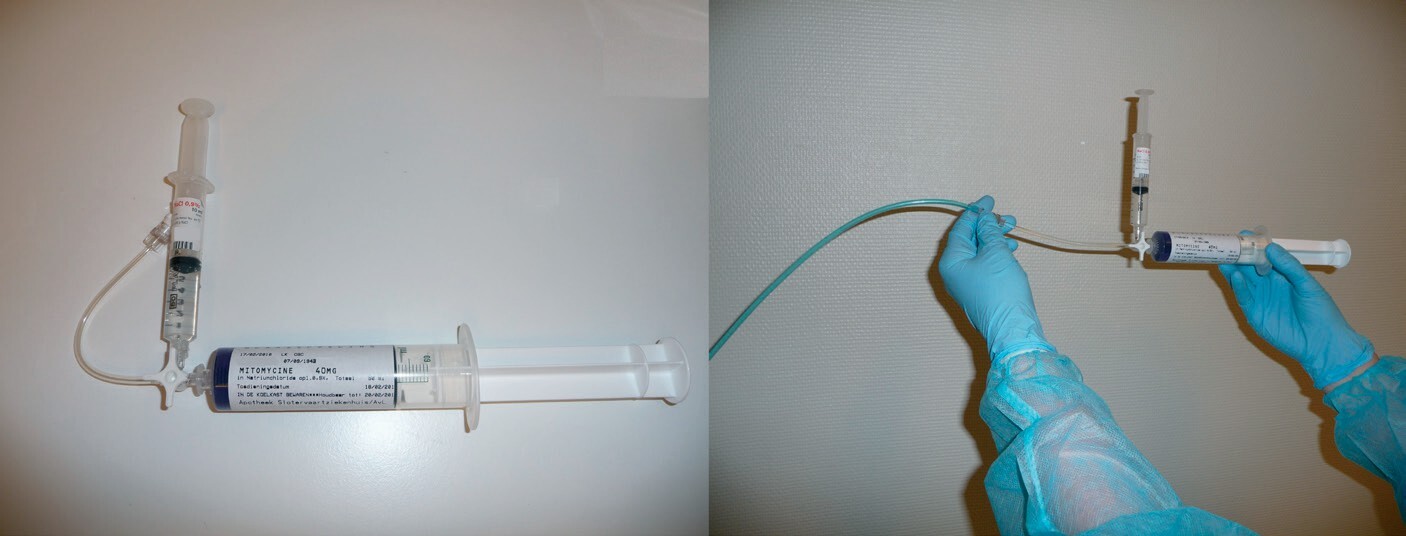
Figure 1: Luer-lock catheter and syringe with MMC
10.6 Recommendations for the preparation and administration of intravesical therapy
| Recommendations | LE | GR |
|---|---|---|
| Do not prepare BCG in areas in which intravenous drugs are prepared. | 3 | B |
| Use an intermittent catheter with the smallest size possible, such as CH10, for intravesical instillations. | 4 | C |
| Use a luer lock catheter to reduce risk of exposure for intravesical instillations. | 4 | C |
| Choose a hydrophilic catheter to reduce risk of discomfort, trauma and infection. | 3 | B |
| Use 10-15ml of lubricant when a non-hydrophilic catheter is used. | 2a | B |
10.7 Ability of the bladder to hold medication
There is no evidence to support the possibility that reduced bladder capacity decreases the effectiveness of intravesical therapy. The total volume of either drug solution is < 60 ml and should be tolerated by any bladder capacity. Factors that may assist patients with reduced bladder capacity to retain these medications for the prescribed dwell time include:
- Minimising the volume of the drug solution to be instilled to increase the concentration in the urine and, therefore, facilitate diffusion across the urinary mucosa [59].
- Treating with anticholinergics.
10.8 Post-operative administration of MMC
The most favourable time for postoperative instillation of MMC is within six hours after TURBT. The rationale for immediate postoperative instillation is:
- Prevention of implantation of circulating tumour cells in the bladder.
- Chemoresection of any residual tumour cells [14].
In a meta-analysis of 18 RCTs (with 3,103 patients), 37% of patients receiving a single dose of MMC chemotherapy immediately after TURBT experienced recurrence, as compared to 50% of those who had undergone TURBT alone [12]. This means that seven patients must be treated to avoid one recurrence. Some authors consider this number an underestimation [11].
10.9 Dwell time
Efficacy of intravesical MMC chemotherapy is relative to the duration of exposure and drug concentration at the tumour site. Dilution of the MMC solution by urine production occurs within five minutes of instillation [74]. Although dwell time is still subject to debate, recurrence rates are lower with an increase in dwell time from 30 to 60 minutes [75]. Systemic drug absorption is not affected by extended exposure to MMC. The dwell time in reported studies were one hour in (range: 25–120 minutes. Although recent RCTs have failed to show significant benefit of a single postoperative instillation, the above-mentioned meta-analysis reported a pooled relative risk of recurrence of 0.67 (95% confidence interval: 0.56–0.79) [12]. If a T1, TIS or Ta high-grade tumour is suspected, the benefit of immediate instillation is not supported by consistent evidence and remains merely an option [76]. In another study administration of the first postoperative instillation later than on Day 0 was associated with > twofold relative risk of recurrence in multivariate analysis [77].
The dwell time that is commonly practised is one hour for Mitomycin and up to two hours for BCG, respectively. Longer periods are not recommended due to dilution of the drug concentration over time as urine is transported into the bladder.
10.10 Patient education
The purpose of education is to empower patients and caregivers, giving them more control and enhancing their ability to solve problems related to intravesical instillation. A key role of nursing is patient education, and many of the nursing interventions described in the study by Wang et al., are related to this role [78]. Both patient education and psychosocial interventions can positively influence the outcome of bladder cancer therapy.
Before beginning any intravesical therapy, patients must be informed about the mechanism of action of their treatment and any potential side effects. Information on scheduling and post-procedural follow-up should also be included. Education should be tailored to both patients and caregivers. The communication skills and attitudes of healthcare professionals play a crucial role in fostering confidence in completing the procedure and encouraging long-term adherence to the treatment plan.
Who: Healthcare professionals need to communicate the procedure to the patient. When patients are discharged, caregivers and those living with the patients require instructions on the precautions needed at home.
When: To decrease anxiety about the treatment, it is important to instruct patients about the necessary steps of the procedure that they are about to undergo. Upon discharge, patients need to know where and when to void, including proper handling of any spilled urine. After discharge, it is important that patients receive counselling regarding signs of local and systemic skin reactions and be instructed to notify their physicians if any of these unforeseen changes occur [78, 79].
Where: Instruction should take place in the clinic prior to any treatment.
How: The educator should make an assessment of the most effective instruction method for each individual patient (i.e. verbal instruction, booklets or digital information). All verbal information should be reinforced with written information that the patients and caregivers can keep and consult.
What: The following topics should be discussed:
- Medications to avoid/delay prior to instillation:
- Antibiotics
- Diuretics
- Fluid intake management:
- Prior to each treatment, fluids should be restricted to maximise the concentration of the drug in contact with the bladder wall. Patients should refrain from fluid intake for eight hours prior to instillation [80]. This minimises urine production during therapy and increases the ability of patients to retain the agent for the prescribed dwell time; usually two hours.
- Upon treatment completion on any day, patients should be instructed to increase fluid intake to flush out any remaining agent from the bladder.
- Voiding post-procedure:
- Upon completion of the prescribed dwell time, patients should void directly into the toilet, and male patients should sit when voiding. This helps limit splashing and contact of surfaces with residual agents.
- After each void, the toilet should be flushed with the lid in the closed position, if available.
- It is common practice in some countries to advise patients undergoing BCG therapy that 250ml of bleach/hypochlorite should be poured into the toilet and remain there for 15 minutes before flushing. However, no evidence has been found to support this recommendation.
- In the case of MMC therapy, due to the possibility of contact dermatitis, patients should be instructed to wash their genitalia after voiding [39].
- The most common side effects associated with BCG and MMC (see Chapter 11).
- Urinary tract irritation is a common reaction to all agents. This may be due to chemical cystitis and not a bacterial infection. Patients should be informed of the signs and symptoms of UTI.
- Launder any clothing that may be contaminated with these agents, through spillage or incontinence, separately from other clothing (see Section 7.5).
- Instruct patients that they may resume normal activity, including health maintenance, diet and exercise for a healthy lifestyle.
- Instruct patients who are sexually active to use barrier/protective mechanisms during intercourse (i.e. condoms) or to abstain from intercourse for one week after treatment.
- Counsel smokers to stop smoking [54].
- Alcohol should be avoided due to its diuretic effect.
For easy reference, these guidelines include a checklist that is intended to assist healthcare professionals to check whether all the information that must be given to the patients has been provided. The checklist for patient information can be found in Appendix 2 - Checklist for patient information.
| Recommendations | LE | GR |
|---|---|---|
| Counsel smokers to stop smoking. | 2a | A |
| Inform patients and caregivers regarding the therapy, fluid intake, safety precautions that should be taken, and any side effects that may occur. | 4 | C |
| Assess the most effective learning method for each individual patient. | 4 | C |